
From the 1Department of Physiotherapy, Faculty of Health Sciences, University of Szeged, 2Department of Medical Physics and Informatics, Faculty of Medicine, University of Szeged, 3Department of Physiotherapy, Faculty of Health Sciences, University of Szeged and 4Department of Orthopedics, Faculty of Medicine, University of Szeged; Doctoral School of Clinical Medicine, University of Szeged, Hungary
#Both these authors charied senior authorship
Objective: To determine the effects of diaphragm-strengthening training on the stability limits of the trunk and inspiratory function in patients with low back pain.
Design: A randomized comparative trial including a diaphragm training group that took part in conventional training together with diaphragm strengthening, and a control group that took part in conventional training only. Both groups participated in an 8-week training, 2 times/week. All subjects underwent the same measurement protocol before and after the intervention.
Patients: The study included 52 subjects with chronic low back pain.
Methods: The inspiratory functions (chest excursion, maximal inspiratory pressure, peak inspiratory flow, and volume of inspired air) and stability limits of the trunk with the subject in the sitting position (modified functional and lateral reach test) were assessed.
Results: Maximal inspiratory pressure and stability limit tests showed a statistically significant improvement only in the diaphragm training group. Statistically significant improvements in chest excursion and peak expiratory flow tests were found in both groups; however, the improvement was more greater in the diaphragm training group.
Conclusion: Conventional exercises together with diaphragm training result in a greater improvement than conventional exercises alone in patients with chronic low back pain.
Key words: low back pain; diaphragm; inspiration; stability limit; postural function.
Accepted Jan 14, 2020; Epub ahead of print Jan 24, 2020
J Rehabil Med 2020; 52: jrm00038
Correspondence address: Regina Finta, Department of Physiotherapy, Faculty of Health Sciences, University of Szeged, Szeged, Hungary. E-mail: fintaregina@etszk.u-szeged.hu
The stability limit of the trunk is reduced in patients with low back pain. The thoracic diaphragm is one of the stabilizer muscles of the trunk. The aim of this study was to assess the effect of diaphragm-strengthening training on inspiratory function and stability limits of the trunk. Fifty-two people with chronic low back pain were included in the study and divided into 2 groups. One group participated in a conventional training programme together with diaphragm-strengthening training, and the other group participated in conventional training only. Both groups underwent 8 weeks of training, 60-min duration, 2 times/week. The results imply that conventional training together with diaphragm-strengthening training may be superior to conventional exercises alone in improving inspiratory function and stability limits of the trunk in patients with chronic lumbar pain.
The diaphragm muscle is a respiratory muscle with postural function (one of the muscles of the local stabilizers of the lumbar spine) and the deep abdominal muscles are postural muscles with respiratory function (1). Synergistic functioning of the abdominal muscles and the diaphragm is needed for postural stability and intra-abdominal pressure, in normal breathing (1). Intra-abdominal pressure can be increased by breath control during a postural task, by controlling the inspired volume of air. Increased abdominal pressure correlates with increased lumbar stability (2, 3). Therefore, segmental instability of the lumbar spine may occur if the respiratory or stabilizer function of the diaphragm or the other stabilizer muscles is reduced, and coordination between the function of the respiratory and postural muscular systems is inaccurate (4). A study by Hagins & Lamberg (4) showed that people with chronic low back pain (CLBP) have different natural breath control from that of healthy individuals. People with CLBP have a higher diaphragm position, a smaller diaphragm excursion (5), and their diaphragm muscle is characterized by greater fatigability (6).
Chronic lumbar pain causes an increased presynaptic inhibition of muscle input (7) and may be associated with diminishing proprioception in muscle spindles (8) causing prolonged latency due to decreased muscle spindle feedback and trunk muscle strength (9). Postural control in healthy subjects is therefore different from that in subjects with lumbar pain (10–12). During prolonged standing, patients with CLBP sway less than healthy subjects in both the anterior–posterior and medial–lateral directions (13). This strategy may be related to the lack of mobility, and might indicate decreased proprioception and lead to a stiffened posture (13). Individuals with low back pain prefer using the ankle strategy to maintain the body in a vertical position (10). A study of individuals with low back pain undergoing inspiratory muscle training showed that, as an effect of the applied training, their postural control changed to a normal, multi-segmental postural strategy (10). The above-mentioned studies assessed postural strategy during standing; several regions of the body (ankles, knees, hips, and trunk) contribute to the values of the measurements in the standing position (14). Reach tests are frequently used to assess dynamic balance and indirectly measure the limits of stability (LOS) (15). However, there is no study of LOS in a sitting position in subjects with CLBP to assess their stability limit. There is a seated version of the reach tests, which is a viable screening tool for seated postural control (16–18) avoiding the ankle strategy.
In an earlier paper we demonstrated that an 8-week diaphragm-strengthening training programme is a viable way to increase the thickness not only of the diaphragm, but also of other stabilizer muscles of the lumbar spine (19). The results suggest that diaphragm-strengthening training may improve trunk stability. The aim of the current study is to evaluate the effect of diaphragm-strengthening training on the parameters of inspiration and to determine whether such training might improve the stability limits of the trunk in patients with non-specific CLBP.
This study is part of a larger research project (registered ID number: NCT03600207). The results describing the effect of diaphragm training on the thickness of the stabilizer muscles have been published previously (19). The current study presents the results related to inspiratory functions and stability limit regarding the 2 main functions of the diaphragm muscle. Therefore, the subjects, the study design, and the training protocol are the same as in the recently published article (19). The new aspects presented in this secondary analysis are described in the “Measurement protocol” section below.
Subjects
Fifty-two subjects with a history of non-specific CLBP were recruited to the study. The inclusion criterion was a history of low back pain for at least 3 months. The exclusion criteria were: diagnosis of a specific cause of low back pain, balance problems with neurological origin, malignant tumour, severe organ diseases, respiratory diseases, a previous surgical intervention that affected the trunk or the extremities, and being an uncooperative subject. Based on these exclusion criteria, 5 subjects were excluded. All participants took part in the study voluntarily, and their written informed consent was gained before the beginning of the first measurement. The study was based on the principles of the Declaration of Helsinki and was approved by the National Medical Research Council (21416-2/2017/EKU). The trial is registered at www.clinicaltrials.gov (identity number NCT03600207). The baseline characteristics of the groups are shown in Table I (19).
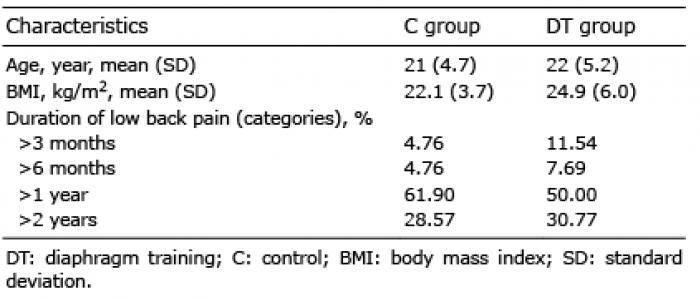
Table I. Baseline characteristics of the 2 groups (19)
Study design
In this randomized controlled trial participants were divided randomly (randomizer.org) into 2 groups. The diaphragm training (DT) group (n = 26) participated in a complex training programme that included conventional exercises together with diaphragm-strengthening training. The control (C) group (n = 21), participated in conventional exercises only. Both groups participated in an 8-week training, 2 times per week, of 60-min duration. Measurements were conducted before and after the intervention period. The study flowchart is shown in Fig. 1 (17). The mean age of the DT group was 22 years (SD 5.2), and the mean age of group C was 21 years (SD 4.7). Mean body mass index (BMI) in group DT was 24.9 kg/m2 and in group C 22.1 kg/m2. There were no sstatistically significant differences between the 2 groups regarding age, BMI, or duration of low back pain (19).
Fig. 1. Study flowchart (19). DT: diaphragm training; C: control; VAS: visual analogue scale; US: ultrasonography; LOS: limits of stability.
Conventional exercise programme
The conventional exercise programme included strengthening, mobilizing and stretching exercises of the trunk muscles. In addition, balance exercises were applied to improve proprioception. The training was divided into 3 parts: warm-up (10 min; breathing and light dynamic exercises for the whole body), main part (40 min; circuit training with 5 sections with 3 min for each +1 min for changing the sections) and cool-down sections (10 min; light dynamic, stretching, and breathing exercises). In the main part static and dynamic balance exercises and combined static and dynamic strengthening exercises for the flexor and extensor muscles of the trunk were applied. Unstable training tools, elastic bands, balls and dumbbells were also used during the training. The exercises were precisely explained and presented, and their implementation was supervised by a physiotherapist. The programme is described in detail in our earlier paper (19).
Inspiratory training
The DT group used an inspiratory muscle strengthening device, POWERbreathe Medic Plus (POWERbreathe Ltd, Warwickshire, UK), which provides resistance during inhalation. The device was used twice a day, in the subject’s own homes, under conditions like 30 inhales per occasion at a speed of 15 inhales/min (10). The device was also used for training sessions during trunk muscle strengthening exercises. The expected inhalation technique for home-based exercises was abdominal breathing in a comfortable positon. To define the amount of resistance during training, the maximal inspiratory pressure (MIP) (in cmH2O) was measured by the POWERbreathe KH2 (POWERbreathe Ltd) device. The resistance was set individually at 60% of MIP (10). The subject wore a nose clip to prevent nasal breathing. At the first meeting the subjects were trained in the correct use of the POWERbreathe Medic Plus device, with the main purpose of the inspiratory load being to strengthen the diaphragm muscle.
Measurement protocol
Measurements were conducted before and after the intervention period. Chest excursion was measured with an inelastic tape at nipple height. The difference between the measurements at the end of inspiration and at the end of expiration was recorded as chest excursion in cm (20).
Inspiratory functions were assessed with the measurement protocols of the POWERbreathe KH2 device. During MIP testing (cmH2O), the patient inhaled maximally against a closed airway from residual volume. The MIP test provides information on the strength of the inspiratory muscles (21, 22). The peak inspiratory flow (PIF) (L/s) reflects the ability of the inspiratory muscles to contract rapidly and to overcome the inherent resistance and elastance of the respiration (22). Functioning of the diaphragm muscle correlates with MIP and PIF values (22). VOLUME (L) is the mean in an upright standing position, and verbal encouragement was given to help the subjects perform maximally. For each patient, the highest value of the inhalation, out of 3 repeat inhalations, was selected for analysis (24, 25).
The stability limit of the trunk was measured with the sitting/modified Functional Reach Test (mFRT) and the modified Lateral Reach Test (mLRT). These tests are reliable measurements to quantify sitting balance and LOS (16). The participant was sitting on a table, with the hips and knees flexed at 90°, and the feet hip-distance apart. The feet were placed on the floor and the back was not supported. Initial reach was measured with the arms flexed at 90°. In the mFRT, the participant was sitting next to a wall (on which a tape measure was fixed) and was asked to reach as far forward as possible. In the mLRT, the measurement protocol was similar, but the participant was sitting with their back against the wall, and was asked to reach as far to the left and right sides as possible. Participants were not allowed to take a step forward or to either side, or to raise their buttocks from the table. Measurement of reach was assessed in cm by the distance between the start and end points. In the mLRT, both the left and the right sides were assessed (17).
Data analysis
Data were analysed in a blinded fashion by comparing group A with group B, without knowing which group was DT and which was C. STATISTICA 13.1 and IBM SPSS Statistics 24 software were used to assess the effect of the intervention and the differences between groups. A Shapiro-Wilk test was used as the normality test. A 2-way repeated measurement analysis of variance (ANOVA) was performed by using the general linear model (GLM) method. There was a within-subject effect (change between before and after training) comparison. For the mean difference of the change, the 95% confidence interval (95% CI) was also calculated. The level of significance was set at p < 0.05.
MIP and LOS tests (mFRT, mLRT) showed statistically significant improvement only in the DT group (p < 0.05). Chest excursion and peak inspiratory flow (PIF) tests show statistically significant improvements in both groups (p < 0.05); however, the improvement was more greater in the DT group. In VOLUME (the mean volume of inhaled air/breath) levels, some improvement was found in both groups (DT and C), but no statistically significant change was found in either group. The results are summarized in Table II, with descriptive statistics and p-values of the pairwise comparisons.
Table II. Results of the statistical comparison
Chest excursion
Mean chest excursion increased by 42.1% in the DT group and by 20.2% in group C as a result of the 8-week intervention (data not shown). The mean difference of the change between the groups was 1.0 cm (95% CI –0.3 to 2.3 cm). The change was statistically significant in both groups (p < 0.05).
Maximal inspiratory pressure
MIP increased in both groups; by 53% in group DT and by 8% in group C. The mean difference of the change between the groups was 27 cmH2O (95% CI 15.5–38.2 cmH2O). The change was statistically significant in the DT group (p < 0.0001), but no statistically significant change was found in group C (Table II, Fig. 2).
Fig. 2. The values of MIP before and after the intervention (mean±SE). *p <0.05. C: control group; DT: diaphragm training group; MIP: maximal inspiratory pressure (cmH2O); SE: standard error.
Peak inspiratory flow
Improvement in PIF was recorded in both groups; PIF increased by 23.0% in the DT group and by 12.0% in group C. The mean difference of the change between the groups was 0.5 L/s (95% CI 0.1–0.9 L/s). The change was statistically significant in both groups (p < 0.001) (Table II, Fig. 3).
Fig. 3. Peak inspiratory flow (PIF) values (L/s) before and after the intervention (mean±SE). *p < 0.05. C: control group; DT: diaphragm training group; SE: standard error.
Mean volume of air inhaled per breath (VOLUME)
Improvement was found in both groups; the VOLUME level increased by 8.2% in the DT group and by 7.3% in group C. The mean difference of the change between the groups was 0.0 L (95% CI –0.28 to 0.35 L). Statistically significant changes were not detected in the DT group (p = 0.07) or group C (p = 0.19) (Table II, Fig. 4).
Fig. 4. VOLUME values before and after the intervention (mean±SE). *p <0.05. C: control group; DT: diaphragm training group; VOLUME: mean of air inhaled per breath; SE: standard error.
Stability limits of the trunk
In mFRT, the DT group improved by 15.8%, while no change was found in group C. The mean difference of the change between the groups was 5.1 cm (95% CI 0.1–9.3 cm). The improvement was statistically significant in the DT group (p < 0.0001) (Table II, Fig. 5).
Regarding the left-sided mLRT, the output improved in both groups; by 14.6% in the DT group and by 3.2% in group C. The mean difference of the change between the groups was 2.3 cm (95% CI –0.004 to 4.7 cm). The change was statistically significant in group DT (p < 0.0001), but not in group C (p = 0.43) (Table II, Fig. 5).
Fig. 5. Results of trunk stability tests before and after the intervention (mean±SE). *p <0.05. C: control group; DT: diaphragm training group; mFRT: modified functional reach test (cm); mLRT-left: left-sided modified lateral reach test (cm); mLRT-right: right-sided modified lateral reach test (cm); SE: standard error.
In the values of the right-sided mLRT the DT group improved by 15.6%, whereas group C improved by 2.0%. The mean difference of the change between the groups was 2.9 cm (95% CI 0.7–5.2 cm). The positive change in group DT was statistically significant (p < 0.0001); however, in group C no statistically significant change was detected (p = 0.62) (Table II, Fig. 5).
MIP and stability limit tests (mFTR, mLRT) showed a statistically significant improvement only in the DT group. Chest excursion and peak inspiratory flow (PIF) tests show statistically significant improvements in both groups; however, the improvement was more greater in the DT group. In VOLUME (the mean volume of inhaled air/breath) levels, some improvement can be seen in both DT and C groups, but statistically significant change is not detectable either group. The main finding of this study is that conventional exercises together with a diaphragm-strengthening protocol (DT group) results in better functional capacity in patients with lumbar pain than conventional exercises alone (group C).
The diaphragm is an essential muscle for breathing; however, it also has a role in preserving the segmental stability of the lumbar spine by maintaining and increasing the intra-abdominal pressure during postural tasks (4). Individuals with low back pain have a disturbed proprioceptive input from the low back area; hence they achieve worse results in the stability limit tests (such as functional and lateral reach tests) than healthy individuals (27). The function of the diaphragm muscle deteriorates if non-specific low back pain occurs (6). In these cases, the diaphragm has a higher position, decreased mobility, and greater fatigability (6). The lumbar range of movement of patients with CLBP with minimal or no pain at the time of measurement is the same as that of the healthy population (28). The mobility of the lumbar area is an influencing factor in the performance of LOS tests (27). It is notable that, despite the more larger decrease in pain in group C (19), group DT showed greater improvement in LOS tests. These results suggest that, as an effect of the diaphragm-strengthening training, both the breathing and the postural functions of the diaphragm muscle have improved. By exercising the diaphragm all the aforementioned dysfunctions may be decreased; a stronger, more mobile muscle (29) may be more effective in increasing the intra-abdominal pressure, and therefore maintaining lumbar stability.
In our previous study of the severity of pain measured by the visual analogue scale (VAS), both training methods resulted in statistically significant improvement (19). Considering the evidence that pain reduces proprioception (30), our results may indicate that the positive change in the severity of pain, together with the increased LOS values, might be a sign of improved proprioception from the lumbar area, represented by better mobility. The deteriorated proprioceptive input might cause postural changes in vertical positions in people with low back pain; individuals tend to lean forward more if low back pain develops (12), and they prefer ankle strategy to the normal multi-segmental strategy for postural control (10, 31). The increased stability limits of the trunk might indicate a more complex postural strategy applied by the DT group. These results are in line with the findings of a former study, describing that improved postural function with the significantly decreased severity of pain may contribute to the normal, multi-segmental strategy in patients with non-specific CLBP (10).
The mobility of the lumbar spine and having strong, well-functioning extensor muscles, are essential to perform the mFRT and mLRT (27). The synergistic function of the global stabilizers (superficial extensors) and local stabilizer muscles (lumbar multifidus, transversus abdominis, pelvic floor muscles, and diaphragm) has a major role during postural tasks (32); for example, during the stability limit tests in our study. It has been demonstrated that reduction in the function of even 1 muscle of the active stabilizer system results in an increased demand on the other subsystems to maintain stability (33); thus, the members of the stabilizer systems influence each other. Our results concerning the inspiratory tests show that the inspiratory function of the diaphragm improved after the 8-week diaphragm-strengthening training. Our previous paper described that the diaphragm-strengthening training might have a statistically significant effect on the stabilizer muscles other than the diaphragm; that is, increased thickness of the muscle belly of the transversus abdominis and lumbar multifidus muscles (19). The significant improvement in functional capacity of the local stabilizer muscles (increased thickness (19) and improved inspiratory function) may result in increased stability limits of the trunk. This finding implies that, in case of non-specific CLBP, an 8-week programme of diaphragm training together with conventional exercises may be superior to conventional exercises alone in improving the functional capacity of the trunk.
Study limitations
A limitation of this study is that the inspiratory manoeuvre applied during MIP and PIF tests is highly effort-dependent (34, 35). However, it has been proven that a co-operative subject can activate the diaphragm maximally during voluntary inspiratory efforts (36). Diaphragm activity was not measured directly in the current study; therefore the accurate value of contraction of the diaphragm was not known when the MIP tests were performed, although verbal encouragement was provided to help the subjects to perform maximally.
Conclusion
As a result of the 8-week diaphragm-strengthening training, the functions of the diaphragm muscle, such as the thicknesses of the stabilizer muscles of the trunk (19), improved significantly, which may result in better postural stability of the lumbar spine and better functioning in people with non-specific CLBP. The importance of non-pharmacological treatments, such as physical exercise programmes, is well-known in reducing the intensity of low back pain (37). Nevertheless, some patients with low back pain are not capable of performing conventional exercises, due to the intensity of the pain or as a result of other medical conditions. Since stability limit and appropriate postural control are the bases of functional capacity (38), diaphragm training may be an appropriate option for these patients to improve their functional level. Moreover, diaphragm-strengthening training might be a favourable additional method for people dealing with the consequences of low back pain, and may also be beneficial in the prevention of non-specific CLBP.
Conflicts of interest.
The authors have a signed loan agreement with the manufacturer of POWERbreathe device (POWERbreathe Ltd.), which is constricted only to the temporary use of the device. No financial support was provided. This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.


 Click to show fullsize
Click to show fullsize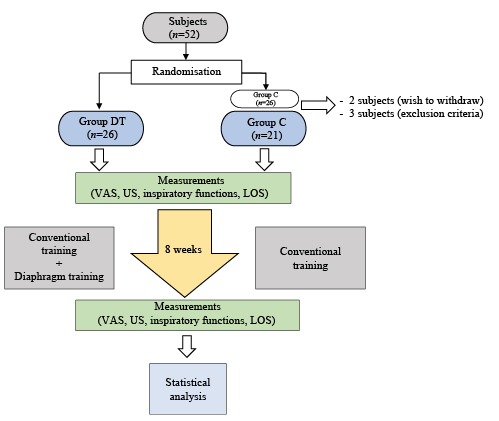 Click to show fullsize
Click to show fullsize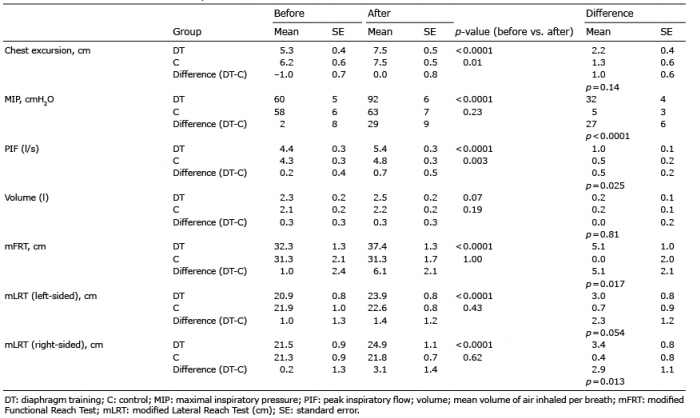 Click to show fullsize
Click to show fullsize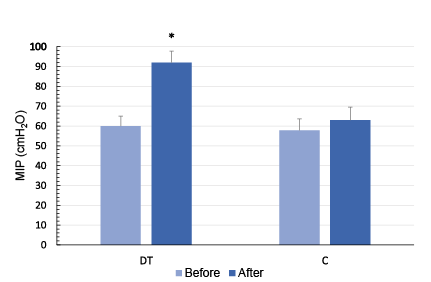 Click to show fullsize
Click to show fullsize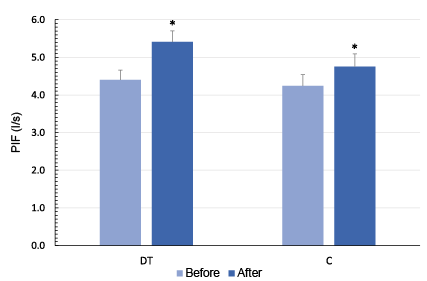 Click to show fullsize
Click to show fullsize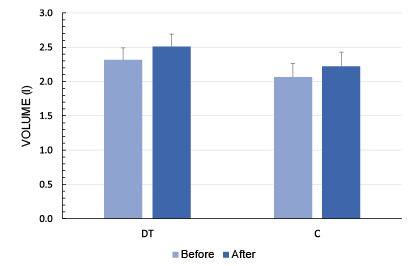 Click to show fullsize
Click to show fullsize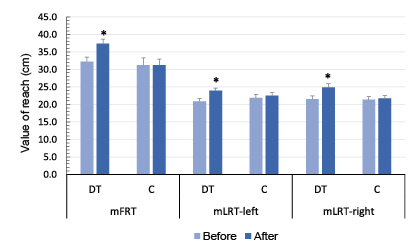 Click to show fullsize
Click to show fullsize